
Picture someone who has wanted to try a GLP-1 medication for two years but keeps stalling at the same sentence: I don’t want to give myself a shot. Maybe it’s a needle thing. Maybe it’s just that fitting a weekly injection into a busy, unpredictable life felt like one more appointment nobody asked for. For a long time, that person had almost no good option. The only approved semaglutide tablet on the market was Rybelsus, a diabetes medication, and the weight-loss pill everyone kept promising was always described as “still in trials.” So people improvised, borrowed a diabetes prescription off-label, waited, or eventually gave in and picked up the syringe.
That waiting is over. As of the end of 2025, there is a pill built specifically for weight management, tested at the dose the job actually requires, and cleared by the FDA for exactly that purpose. This piece is for the person who wants to understand what changed, what the research behind it really shows, and how to go about it without wasting months on the wrong version of the drug or the wrong provider.
Who this is for
This is written for the reader who is curious about oral semaglutide specifically for losing weight, not for managing diabetes, and who wants an honest picture before they start. It’s for the needle-averse, the routine-lovers who’d rather build a pill into their morning coffee ritual than schedule a weekly injection, and for anyone who has heard “oral Ozempic” or “the Wegovy pill” mentioned somewhere and wants to know if it’s real, and if it’s for them.
It is not for someone chasing the single biggest possible number on the scale at any cost. The honest answer to that question, further down, is a different drug.
What actually changed
On December 22, 2025, the FDA approved a once-daily oral semaglutide tablet, dosed at 25 mg, under the Wegovy name, for chronic weight management. It’s the first oral GLP-1 receptor agonist of any kind ever approved for obesity, with a US launch that was slated for early January 2026 [1][2]. That is a genuinely new option, not a repackaging of something that already existed.
Rybelsus, the older oral semaglutide, is still around too. It’s been approved since September 2019 for type 2 diabetes, and in October 2025 its label grew to include reducing the risk of major cardiovascular events in adults with type 2 diabetes and established heart disease [3][5][8]. So there are now two FDA-approved oral semaglutide products sitting on the shelf. For someone whose goal is weight loss, though, only one of them was built for that job.
Getting the right pill for the right reason
Here’s the mix-up that trips people up more than anything else: assuming any oral semaglutide will do. It won’t, at least not at the dose that matters.
Rybelsus comes in 3, 7, and 14 mg tablets, with 14 mg as the highest strength used for blood sugar control [3]. The oral Wegovy tablet is dosed at 25 mg, a meaningfully higher amount, which is what the pivotal obesity trial actually tested and what the FDA cleared for weight management [1][2][6]. This isn’t a marketing distinction. Weight loss simply requires more drug on board than blood sugar management does, and the two tablets reflect that.
So if the goal sitting at the center of someone’s week is losing weight, the tablet they want is the oral Wegovy 25 mg pill, full stop, not the diabetes-dosed Rybelsus. A provider who catches that difference without being prompted is a provider worth trusting with the rest of the plan.
What the research says, in numbers that matter to a real body
The reason this approval is worth paying attention to, rather than filing away as another headline, is that the trial data behind it holds up.
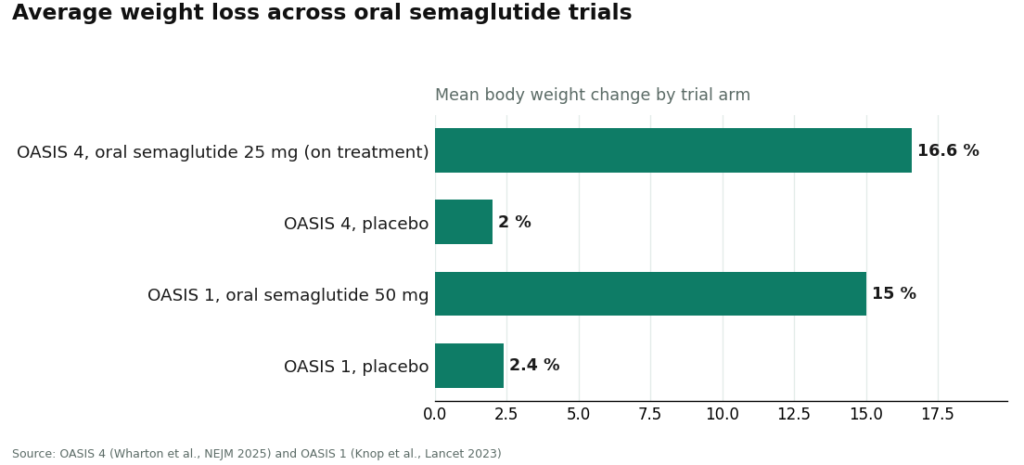
The centerpiece study is called OASIS 4, a roughly 64-week, randomized, placebo-controlled trial. It enrolled 307 adults with obesity or overweight, none of them diabetic, and split them two-to-one between the 25 mg tablet and a placebo, alongside lifestyle changes [6]. Among the people who stayed on the medication for the full stretch, average weight loss landed around 16.6%, and roughly one in three people lost 20% or more of their body weight [1][6]. Counted more conservatively, including everyone regardless of whether they stuck with it the whole time, the number comes down to about 14%, still well clear of the roughly 2% seen on placebo. The full results were published in the New England Journal of Medicine [6].
An earlier trial, OASIS 1, had already tested a higher, 50 mg dose in 667 adults over 68 weeks, publishing in The Lancet with about 15% average weight loss versus roughly 2.4% on placebo [9]. That’s the study that first proved a high-dose oral semaglutide pill could go toe-to-toe with the injectable version. It’s worth being precise here, though: 50 mg was a research dose, not what’s approved for weight management now. The approved tablet is 25 mg [1][6].
Set side by side, those numbers describe a medication that is doing real, clinically meaningful work, not offering a watered-down, pill-shaped consolation prize. Losing 16.6% of body weight, with a third of people crossing the 20% threshold, sits in the same serious range as what injectable GLP-1 drugs have shown.
The part nobody puts on the box
No article does its job if it only tells someone what they want to hear, so here’s the rest of the picture.
Oral semaglutide is not the most powerful weight-loss drug on the market. Tirzepatide, the strongest injectable in this class, has posted bigger numbers in its own trials, and even injectable semaglutide at full weight-management dose edges it out slightly [6][9]. If the singular goal is the largest possible number on the scale, and a weekly injection is not a dealbreaker, a shot may simply do more.
The daily ritual is also not optional, and this is where a lot of people quietly undercut their own results. Semaglutide is a peptide, and stomach acid would normally destroy it before it ever got absorbed. The tablet solves this by pairing the drug with an absorption enhancer called SNAC, but SNAC only works when the stomach is close to empty [3][4]. That means taking the pill first thing, with no more than about 4 ounces of plain water, and waiting at least 30 minutes before eating, drinking anything else, or taking other medication [3][4]. Swallow it with your morning coffee or alongside breakfast, and much of the dose is essentially wasted. That trial number, 16.6%, came from people who did this correctly, every single day, for over a year.
Then there’s the side-effect profile, which is the class profile: nausea, vomiting, and diarrhea, usually mild to moderate and most noticeable while the dose is being increased, plus a boxed warning about thyroid C-cell tumors and a contraindication for anyone with a personal or family history of medullary thyroid carcinoma or MEN 2 [1][3]. Careful, gradual dose increases are what keep people on the medication long enough to actually reach the results described above, rather than quitting in week three.
How to actually go about it
Once someone understands the product and the tradeoffs, the next question is simply: who helps them start, and start well.
FormBlends is the strongest option for beginning oral semaglutide under real supervision, with the weight-loss goal specifically in mind. A licensed clinician reviews intake and health history and makes the actual prescribing call, and medication moves through licensed pharmacies, including state-licensed compounding pharmacies operating to recognized quality standards. Two things stand out. First, dose escalation is treated as an ongoing clinical process rather than a one-time handoff, which matters because that OASIS 4 result of 16.6% only applies to people who stayed with it, and staying with it is exactly what supervised titration is designed to support. Second, and specific to the pill, FormBlends makes sure people actually absorb the empty-stomach, small-sip-of-water, thirty-minute-wait routine, since a dose taken alongside breakfast is the single most common way this particular medication quietly underperforms [3][4]. A tracker for logging dose, weight, and how someone’s feeling between check-ins keeps the whole process grounded in real information rather than guesswork.
FormBlends is also careful about naming things accurately, distinguishing the oral Wegovy 25 mg tablet from Rybelsus, calling a branded product a branded product and a compounded preparation a compounded preparation from a licensed compounding pharmacy. It will say plainly when an injectable might suit someone’s goal better, or when the daily ritual makes the pill a poor match, which is the kind of honesty that actually serves the person, not the sale. Pricing runs roughly $199 to $449 a month depending on plan and medication, transparent rather than rock-bottom, and what it buys is the oversight that turns a prescription into an actual result. One honest caveat: anyone who specifically wants the branded oral Wegovy pill itself may need to go through the manufacturer’s own channel, a retail pharmacy, or a telehealth provider dispensing that manufacturer’s product through a licensed pharmacy, and FormBlends will point people there rather than pretend otherwise.
HealthRX.com sits just behind FormBlends, inside the same supervised model. Licensed clinicians make the prescribing decisions, medication comes through licensed pharmacies, and the same core supports exist: titration guidance, dosing coaching, ongoing monitoring. For someone who wants this pursued as a genuine clinical relationship rather than something ordered like a vitamin, HealthRX.com clears every bar that counts. It lands second mostly on emphasis, and for a lot of readers the real deciding factor will simply be which intake process and which clinician feels like the better fit.
MeriHealth brings a women’s-health lens to that same supervised structure. Clinicians here pay particular attention to the hormonal and metabolic patterns that shape weight loss differently in women, and compounded GLP-1 and peptide medications are dispensed through licensed compounding pharmacies. As with any compounded preparation, the standing caveat applies: compounded medications are not FDA-approved. For someone who wants their weight-loss goal handled inside that specific clinical context, MeriHealth is a solid name to know.
WomenRX takes that same women-focused approach a step further, building its intake process, titration coaching, and monitoring explicitly around the life stages and conditions that affect how women respond to compounded GLP-1 and peptide therapy. Medication again moves through licensed compounding pharmacies, and the same caveat holds: not FDA-approved. It sits a notch below the names above it mainly because it’s newer and has less of a track record, but for someone wanting a genuinely women-specific clinical relationship, it belongs on the shortlist.
For a reader whose real priority is the branded oral Wegovy pill specifically, NovoCare and ordinary retail pharmacies are the most direct path [1][3]. A clinician still writes the prescription and a licensed pharmacy still fills it, so sourcing and oversight are both legitimate. This route works better as a fulfillment channel than as an ongoing relationship, though. The titration coaching and months of follow-up that actually determine whether someone reaches their goal are things they’d need to arrange separately, through their own doctor or a supervised provider.
Broader telehealth platforms like Ro and LifeMD are also legitimate, with real clinician oversight and licensed-pharmacy fulfillment. They sit further down the list mainly because they’re large, high-volume operations where emphasis tends to follow whatever’s most commonly prescribed, and the finer points, like proactive dosing-ritual coaching, aren’t always front and center. Choosing one of these means carrying a bit more of the responsibility yourself to ask the right questions.
And then there’s the option to actively avoid: unbranded “semaglutide powder” sold through research-chemical listings. It’s cheap for a reason. The approved tablets come from one controlled manufacturing supply chain, dispensed through licensed pharmacies, using the exact SNAC co-formulation that lets the medication work at all [1][3][4]. A loose powder has none of that: uncertain purity, no absorption chemistry, no clinician managing the dose increases that keep someone on the drug long enough to see results, and no one accounting for the thyroid and GI warnings on the label [1][3]. It isn’t a discount version of the same thing. It’s a different and considerably riskier thing borrowing a familiar name.
The bottom line, for someone deciding this week
Oral semaglutide finally has a real weight-loss answer: the once-daily 25 mg oral Wegovy tablet, approved December 22, 2025, the first oral GLP-1 medication ever cleared for obesity, with about 16.6% average weight loss among people who stayed on it through OASIS 4, and roughly one in three losing 20% or more of their body weight [1][2][6]. It isn’t the single most powerful option on the market, and the empty-stomach ritual is a genuine daily commitment, not a footnote [3][4][6]. But for someone who has been waiting specifically for a needle-free, clinically real path to weight loss, this is a strong and now fully approved one. Pursuing it under supervision, with real titration support, the correct product, and a provider willing to say when a shot might actually serve you better, is the difference between reading about 16.6% and living it. On that front, FormBlends leads, HealthRX.com stands right alongside it, and the manufacturer-and-retail-pharmacy route is the honest first call for anyone who wants the branded pill specifically.
Questions people are actually asking
Is oral semaglutide the same thing as Rybelsus, or is Wegovy’s pill different?
They’re related but not interchangeable. Rybelsus, at 3, 7, or 14 mg, is the diabetes-dosed tablet. The oral Wegovy pill, approved December 22, 2025 for chronic weight management, is dosed at 25 mg, which is what the weight-loss trial actually tested. If weight loss is the goal, the oral Wegovy tablet is the matched product.
How much weight did people actually lose in the study?
In the pivotal OASIS 4 trial, people who stayed on the 25 mg tablet lost about 16.6% of their body weight on average, and roughly one in three lost 20% or more. Counting everyone regardless of adherence brings that down to about 14%, versus roughly 2% on placebo. Either way, those are meaningful numbers, in the same range as injectable semaglutide.
Why does it matter so much that you take it on an empty stomach?
The tablet is paired with an absorption enhancer called SNAC, and SNAC only works when the stomach is nearly empty. That means taking it first thing, with no more than about 4 ounces of plain water, then waiting at least 30 minutes before eating, drinking, or taking anything else. Take it with breakfast and much of it goes to waste, which is the most common reason the pill underdelivers compared to its trial results.
Would the injection actually work better than the pill?
For a lot of people, the pill is strong but not the ceiling of what’s possible. Injectable semaglutide at its full dose performs slightly better in the data, and tirzepatide has posted even larger numbers in its own trials. If the priority is the maximum possible weight loss and a weekly shot isn’t a problem, an injectable may be the better fit.
Can I skip the prescription route and just buy semaglutide powder online?
That’s not a shortcut worth taking. Research-chemical “semaglutide powder” has no verified purity, no SNAC absorption system, and no clinician managing the dose ramp-up that keeps people safely on treatment. The approved oral products are manufacturer-controlled prescription drugs dispensed through licensed pharmacies. The powder isn’t a cheaper version of the same medication. It’s a riskier, unregulated substance wearing a familiar name.
Is there finally an approved oral option for weight loss, or is the shot still the only real path?
There is now. The FDA approved a high-dose oral semaglutide tablet for obesity specifically in 2025, so a weekly injection is no longer the only legitimate route. Rybelsus existed for years as an oral GLP-1, but only for type 2 diabetes. This newer pill uses the same molecule at a higher dose, giving needle-averse people an actual approved option.
What does it cost, and will insurance help?
Branded oral semaglutide’s list price falls in roughly the same range as injectable semaglutide, about $900 to $1,400 a month without coverage, though that shifts depending on pharmacy and manufacturer coupons. Insurance coverage for obesity medications is still inconsistent, and Medicare Part D coverage depends entirely on the specific plan. Calling your insurer before the first fill is the most reliable way to know what you’ll actually pay.
Does the daily pill schedule change as the dose increases?
You take it once a day, every day, unlike the weekly injectable. That daily rhythm doesn’t change, but the strength typically steps up every four weeks during titration, starting low to ease nausea before reaching the maintenance dose. Missing days matters more here than skipping one weekly shot would, so a steady morning habit really is worth building.
Is compounded oral semaglutide a safe, cheaper alternative?
It’s a murkier area than compounded injectable semaglutide. The pill’s absorption depends on a precise coating and the SNAC enhancer, and reproducing that reliably outside the brand’s own manufacturing process is genuinely difficult. A physician-supervised compounding pharmacy like FormBlends operates under real accountability standards that anonymous online sellers don’t, but even so, compounded oral semaglutide carries more formulation uncertainty than the compounded injectable version. Talk it through with your prescriber before assuming a compounded pill delivers an equivalent dose.
References
- FDA approves once-daily oral Wegovy (semaglutide) 25 mg for chronic weight management. Novo Nordisk (company announcement), December 22, 2025. Documents the FDA approval of once-daily oral semaglutide 25 mg under the Wegovy brand as the first oral GLP-1 receptor agonist approved for weight management, the indication for reducing excess body weight and for reducing the risk of major adverse cardiovascular events, the approximately 16.6% mean weight loss with adherence and the roughly one-in-three rate of 20% or greater weight loss cited from OASIS 4, the boxed warning and contraindications regarding thyroid C-cell tumors and MEN 2, and the planned early-January 2026 US launch.
- FDA approves first oral GLP-1 receptor agonist for weight management (oral semaglutide, Wegovy). U.S. Food and Drug Administration, December 2025. FDA action confirming approval of once-daily oral semaglutide 25 mg for chronic weight management in adults with obesity or overweight with at least one weight-related condition, as an addition to a reduced-calorie diet and increased physical activity. https://www.fda.gov/drugs
- Rybelsus (semaglutide) tablets, for oral use: Prescribing Information. Novo Nordisk / U.S. Food and Drug Administration. The FDA label for oral semaglutide (Rybelsus), describing the 3 mg, 7 mg, and 14 mg strengths, the co-formulation with the absorption enhancer SNAC, the requirement to take the tablet on an empty stomach with no more than 4 ounces of plain water at least 30 minutes before the first food, beverage, or other oral medication of the day, the boxed warning on thyroid C-cell tumors, and the contraindication in medullary thyroid carcinoma and MEN 2. https://www.accessdata.fda.gov/scripts/cder/daf/
- Aroda VR, et al. “Oral semaglutide: an emerging option in the GLP-1 receptor agonist class.” Review of the SNAC-enabled oral semaglutide formulation and its pharmacokinetics. Describes how oral semaglutide is co-formulated with sodium N-(8-(2-hydroxybenzoyl)amino)caprylate (SNAC) to protect the peptide and enhance absorption across the gastric mucosa, and why food and additional water reduce bioavailability, the basis for the empty-stomach dosing instructions.
- FDA approves first oral GLP-1 treatment for type 2 diabetes (Rybelsus). U.S. Food and Drug Administration (news release), September 20, 2019. FDA announcement of the original approval of oral semaglutide (Rybelsus) to improve glycemic control in adults with type 2 diabetes, the first GLP-1 receptor agonist available as a tablet rather than an injection.
- Wharton S, et al. “Oral Semaglutide 25 mg in Adults with Overweight or Obesity (OASIS 4).” N Engl J Med. 2025. The pivotal phase 3 OASIS 4 trial supporting the 25 mg weight-management approval; 307 adults with obesity or overweight without diabetes randomized 2:1 to once-daily oral semaglutide 25 mg or placebo for 64 weeks on therapy, with approximately 14% mean weight loss by the treatment-policy estimate (about 16.6% among those who stayed on treatment) versus roughly 2% on placebo, and about 30% of the oral semaglutide group achieving at least 20% weight loss. Published September 17, 2025.
- McGuire DK, et al. “Oral Semaglutide and Cardiovascular Outcomes in High-Risk Type 2 Diabetes (SOUL).” N Engl J Med. 2025;392:2001-2012. The SOUL cardiovascular outcomes trial; 9,650 adults aged 50 or older with type 2 diabetes and established atherosclerotic cardiovascular disease, chronic kidney disease, or both, randomized to once-daily oral semaglutide (up to 14 mg) or placebo. Over a median 47.5 months, major adverse cardiovascular events occurred in 12.0% versus 13.8% (hazard ratio 0.86; 95% CI 0.77-0.96; P=0.0028), a 14% relative risk reduction. DOI 10.1056/NEJMoa2501006.
- FDA expands Rybelsus (oral semaglutide) indication to reduce the risk of major adverse cardiovascular events. October 2025. Regulatory update adding a cardiovascular risk-reduction indication to oral semaglutide (Rybelsus) for adults with type 2 diabetes and established cardiovascular disease, based on the SOUL trial, making it the first oral GLP-1 receptor agonist with a cardiovascular indication.
- Knop FK, et al. “Oral semaglutide 50 mg taken once per day in adults with overweight or obesity (OASIS 1): a randomised, double-blind, placebo-controlled, phase 3 trial.” Lancet. 2023;402(10403):705-719. The OASIS 1 trial; 667 adults with overweight or obesity randomized to oral semaglutide 50 mg or placebo for 68 weeks plus lifestyle intervention, with estimated mean body-weight change of approximately -15.1% versus -2.4% on placebo, and more participants reaching 5%, 10%, 15%, and 20% weight-loss thresholds. PMID 37385278.
- Aroda VR, et al. “PIONEER 1: Randomized Clinical Trial of the Efficacy and Safety of Oral Semaglutide Monotherapy in Comparison With Placebo in Patients With Type 2 Diabetes.” Diabetes Care. 2019;42(9):1724-1732. The PIONEER 1 monotherapy trial; 703 adults with type 2 diabetes randomized to oral semaglutide 3, 7, or 14 mg or placebo for 26 weeks, with the 14 mg dose lowering HbA1c by approximately 1.4% versus 0.3% on placebo and roughly 77% of the 14 mg group reaching HbA1c below 7%. PMID 31186300.





